On the rare occasions when a child is too small to sit by themselves, or they are too frightened to allow me to examine them there comes a moment, when we need to decide:
Whether and how to proceed with the physical examination.
Do we go ahead?
We need to ask ourselves how important the examination really is at this moment. And sometimes it just is necessary to go ahead. But then it should be worth the effort for us and potential trauma for the child.
But how?
If we really need the examination, the next question would be: how?
In this situation, we have to assess whether the present parent or next of kin is suitable to hold the child during the process of physical examination.
Who is the optimal supporter?
If the parent is too terrified themselves, or if they still show non-verbally that they mistrust us, they would not be suitable for this “supporting” role.
In those cases, a medical student or a nurse might actually be the better choice.
How to fight with the child?
The most frequently used pose is, that the child sits or stands between the legs of the supporting person, facing the examiner frontal and the supporter wraps one arms around the child’s arms and holds the head with the other arm.
This pose is very ineffective because the child still can wriggle quite frantically, making any meaningful interactions almost impossible.
Is there a better way?
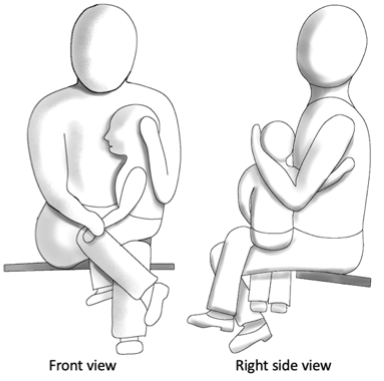
An efficient way in how to hold the child on the supporting person’s lap is shown in the drawings below.
They show a very effective way to control the child’s legs, arms and head for the ENT-examination. And this position would also be good for bleeding of children.

Let’s break this down:
How to physically support a child:
- The child is placed sitting sideways on one knee on the lap of the adult.
- The legs of the child are placed between the adult’s legs. This prevents the child from kicking.
- The legs of the child are secured by the adult person’s legs.
- The bottom of the child is placed as close as possible to the adult’s hip. This prevents sideways wiggles.
- The arm of the child that is close to the adult is slid around the waist of the adult, reaching to the back underneath the shoulder of the adult.
- The head of the child rests against the adult’s chest and is held in place by the adult’s hand that is close to the child’s back.
- The other hand of the child is held down at the wrist by the other hand of the adult.
This position allows assessment of one ear, the nose, and the mouth of the child.
For the other ear, the child is placed the other way around on the other knee.
This position is possible from neonatal age until about 10 years of age.
In case that it would be possible, I would often prefer for a nurse or medical student to hold the child rather than the parents. The reason is, that the proximity with parents should remain a safe place for any child in a stressful situation.
In a nutshell:
If you need to physically support a child for a procedure, do it in a quick and efficient manner.
Previous post Next post
Podcast Real – life video Patient-feedback
Connect Respect Engage Extra tips Contact/About me
Communication lives on comments … fancy to share yours?